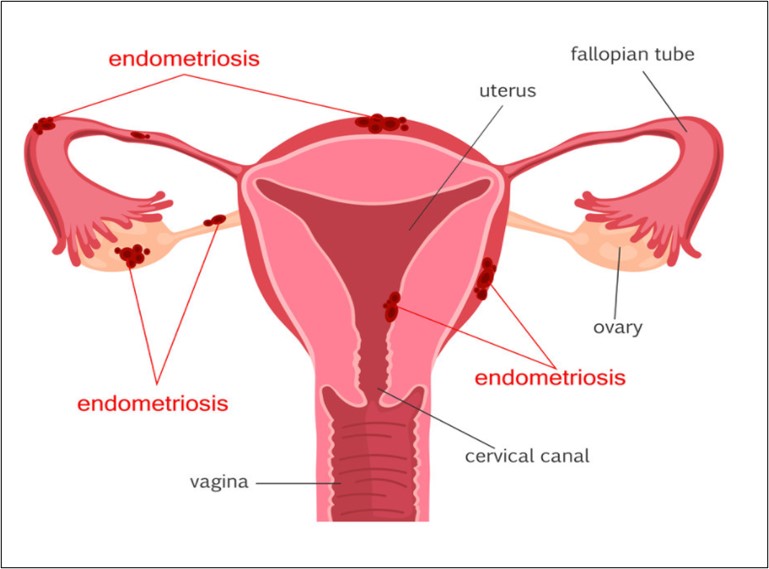
Endometriosis affects 176 million women around the globe. Endometriosis is a chronic condition that occurs when tissue that lines a woman’s uterus, called the endometrium, starts to spread in other parts of the body, such as within the pelvis, ovaries, fallopian tubes, uterus and bladder. Common symptoms include dysmenorrhoea, dyspareunia, non-cyclic pelvic pain, and subfertility. The name of this condition is derived from the word "endometrium" which is the tissue that lines the uterus. During menstruation, endometrial tissues arrive in the abdominal cavity through the fallopian tubes, adhere to the peritoneal lining and develop into endometriotic lesions.
Although the exact cause of endometriosis is still not known, it is highly likely that specific genes predispose women to develop the disease. Thus, women are at high risk of developing endometriosis if their mother and/or sister are also affected. During menstruation, hormones cause the lining of the uterus to thicken in preparation for a possible pregnancy. When the egg does not get fertilized, the tissue breaks down and exits through the vagina. Endometriosis happens when those hormones trigger similar thickening and bleeding in the tissue growing outside the uterus. This often makes women bleed more during the period, but not always. It is an enigmatic disease that could start at birth.
Types of Endometriosis
i. Superficial Peritoneal Endometriosis: This is the most common type of endometriosis. Small deep lesions involve the peritoneum. The lesions do not invade the space underlying the peritoneum.
ii. Cystic Ovarian Endometriosis: Sometimes, women with endometriosis can develop endometrioma in their ovaries which is considered as most potential threat to a woman’s reproductive potential. Ovarian endometrium forms dark fluid-filled cavities called cysts or endometrioma. The cysts are known as chocolate cysts.
iii. Deep Endometriosis: The least common subtype of endometriosis is deeply infiltrating endometriosis. It is so named because it is found deep within the tissue or organ. In this type of endometriosis, lesions invade organs that are near the uterus and beyond the surface of the peritoneum.
Causes & Symptoms of Endometriosis
The causes of endometriosis are still unclear. One theory suggests that some of the endometrial tissues pass back through the fallopian tubes into the pelvic cavity during menstruation along with menstrual blood. This is known as retrograde menstruation. Another theory states that endometrial tissue may travel and implant via blood or lymphatic channels and spread like cancer cells. A third theory suggests that cells lining the pelvic organs may transform into endometrial cells.
The symptoms of endometriosis include excessive menstrual cramps, pain during intercourse, heavy menstrual flow, infertility, painful urination, painful bowel movements and gastrointestinal problems.
Endometriosis and Infertility
Endometriosis is associated with an increased risk of infertility. It is thought that endometrial tissue can inhibit the release of the egg from the ovary and distorts the fallopian tube so that they are unable to pick up the egg after ovulation, thus making it difficult for the sperm to meet the egg. Impaired implantation of the fertilized egg is another cause of infertility.
Treatment
Endometriosis is a chronic disease. Currently, there is no known cure for endometriosis, but the symptoms can be managed by different treatment options. Treatment for endometriosis may include:
i. Pain medications: Nonsteroidal anti-inflammatory drugs are the first-choice drugs such as ibuprofen, naproxen or other over-the-counter analgesics, can help reduce endometriosis pain.
ii. Hormonal Therapy: Hormone therapy can be used to treat endometriosis-associated pain. These treatments stop the ovaries from producing hormones and prevent ovulation. This therapy includes
a) Oral Contraceptives: A combination of estrogen and progestin hormones prevents ovulation and reduces menstrual flow.
b) Progestins: If oral contraceptives start showing side effects, often a progestin is given as second-line therapy. Progestin inhibits estrogen and the growth of the endometrium. They may have more side effects than an oral contraceptive.
c) Gonadotropin-releasing hormone (GnRH) agonist: GnRH medicines stop ovarian hormone production, creating a sort of “medical menopause”. For example: Lupron stops the production of estrogen and progestin and is highly effective at relieving endometriosis. They are given by injection.
d) Danazol: Danazol is a hormone derived from the male hormone testosterone. It also can be very effective at reducing endometriosis by stopping the release of hormones responsible for the menstrual cycle. However, it may cause side effects such as hair growth or acne.
iii. Surgical Treatments: Sometimes, surgical techniques may provide short-term relief from endometriosis-associated pain. Surgical treatments include laparoscopy, laparotomy and hysterectomy (surgical removal of the uterus).
Lifestyle changes pose a significant impact on endometriosis. Increased physical activity, drinking plenty of water, quitting smoking, avoiding drinking alcohol and caffeine may reduce the risk of endometriosis. Additionally, an early diagnosis and treatment can prevent the development of endometriosis. Besides conventional strategies, new therapies will likely be introduced in the coming years. Given that endometriosis is common amongst women during reproductive life span, it is imperative that quality research continues to be executed so that this disease may be better understood and optimally treated.