
SARS-CoV-2 infection is a double challenge faced by the people inhabiting cancer. Covid-19 pandemic has significantly posed a challenge in the management of patients, especially with lung cancer, and had raised a million-dollar question “how?”. Scientists and medical personnel are sweating on their feet to manage and bring the situation under control and they have come a long way with their hard work. Why only scientists and doctors? We are also equally responsible for the control of this pandemic situation. Before that, it is important to know the cause, symptoms, and management of SARS-CoV-2, especially in comorbid situations like lung cancer. Though, it is not possible for a common man to know everything but must remain aware of the possible risk factors associated with complications such as old age, significant respiratory and cardiovascular distress, smoking-related lung diseases, poor nutritional status, and immunosuppressive treatment. Till now, the novel coronavirus which originated from Wuhan in China, also known as SARS-CoV-2, or popularly known as COVID-19, has received its fame due to causing the current pandemic that became a significant health problem worldwide. The overlap between the radiological manifestations and the CT findings of SARS-CoV-2 induced pneumonia is critical for the management of lung cancer patients because they are more prone to any opportunistic infections.
Where Lies the Similarity?
SARS-CoV-2 specifically binds to the angiotensin I converting enzyme-2 (ACE2) receptor present in the alveolar epithelial cells is the cause for lung infection so, isn’t it a double risk factor for a lung cancer patient? Many a time the presence of ACE2 receptor in other organs becomes the cause for multi-organ failure. The worsening of pulmonary symptoms during lung cancer progression is found to be similar to that of COVID-19, further adding typical complexity in the course of disease in lung cancer patients.
What happens inside our body?
Coronaviruses are crown-like particles with spikes protruding from their surface. They are enveloped viruses with single-stranded, positive-sense RNA (+SSRNA) genomes of approximately 26-32 kb. They break all the immune barriers of the human body and hence become successful in constructing their own home hindering the host’s physiological and biological processes. Mainly it recognizes and binds (10 times more strongly) to the ACE2 receptor found in the lungs and other organs of the body, where transmembrane serine protease-2 (TMPRSS2) acts as a support. It takes minimum incubation period of 14 days to manifest the symptoms.
The phases of infection occur as:
Phase 1: Cell invasion and viral replication in the nose.
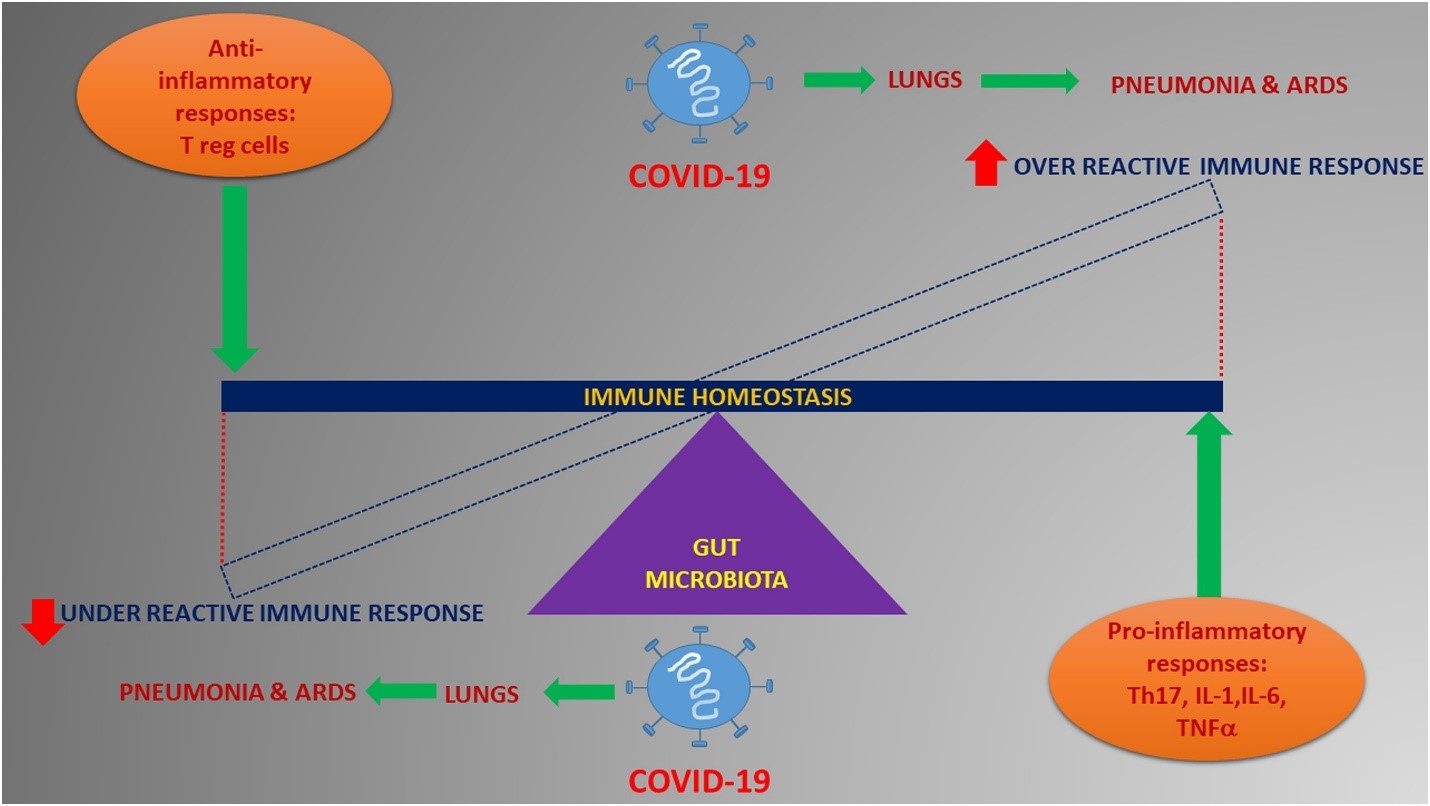
Phase 2: Replication in lung and alteration of the immune system.
Phase 3: Pneumonia.
Phase 4: Acute respiratory diseases syndrome, the cytokine storm and multiple organ failure.
Interesting Part: The angiotensin-converting enzyme 2 (ACE2) receptor, which allows SARS-CoV-2 to enter the body, is also considered as the key enzyme in the protection of lungs in the later phases of the disease.
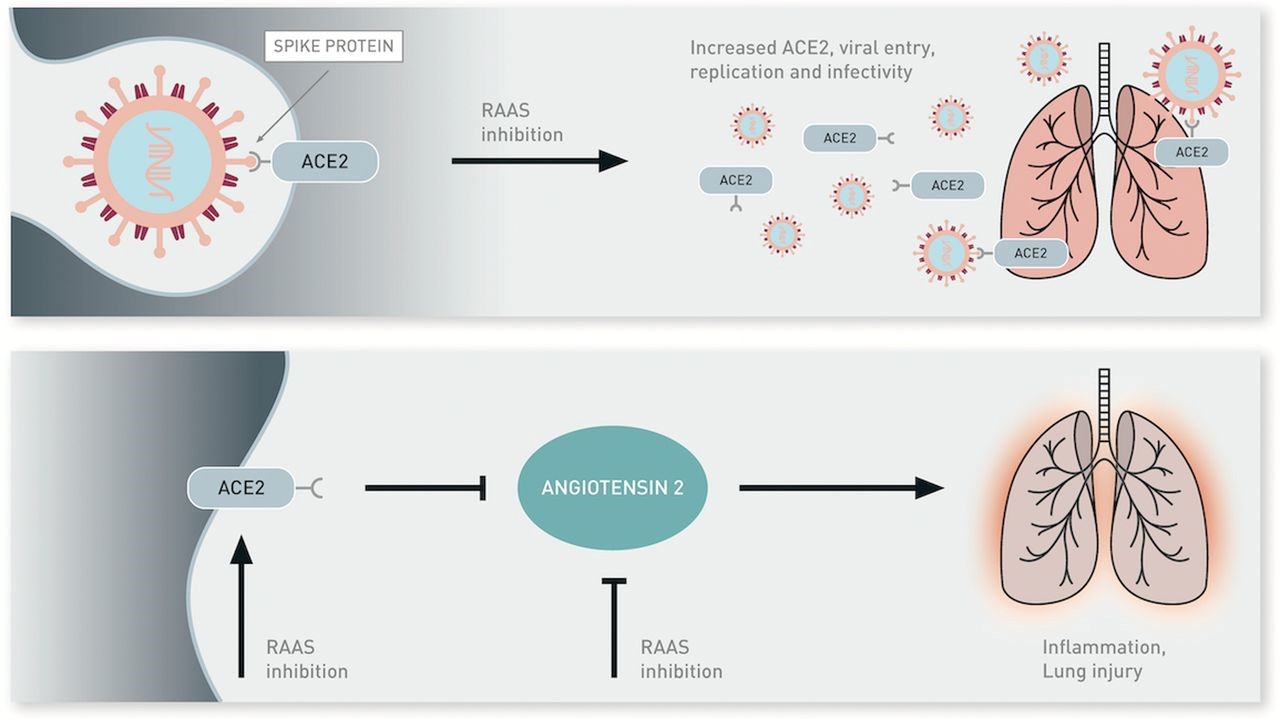
What helps ACE2 regulation?
It is renin-angiotensin-aldosterone system (RAAS) whose inhibition may up-regulate ACE2 expression and consequently increasing viral entry and replication. ACE2 reduces levels of angiotensin II, which is a potent pro-inflammatory agent in the lungs and can contribute to lung injury. RAAS inhibitors may block the production or function of angiotensin II and increase potential levels of ACE2, hence indirectly inhibiting angiotensin II.
Therapeutic Approaches
Several investigational treatments were administered, including hydroxychloroquine, azithromycin, remdesivir, tocilizumab, convalescent plasma, and corticosteroids due to the absence of any approved therapy for SARS-CoV-2. Different approaches like immune checkpoint inhibitors have largely impacted the prognosis of a multitude of malignancies with significant improvement in survival outcomes. Various Chinese trials have assessed the role of the anti-VEGF bevacizumab, the myeloma drug thalidomide, the PD-1 inhibitor camrelizumab and other anti-cancer agents in the treatment of SARS-CoV-2 infections.
How Important is Management?
Diligent and judicious management of cancer patients with SARS-Cov2 could guarantee a better outcome for these patients. To minimize the number of hospital visits due to high transmissibility rate for SARS-CoV-2, and prevent anti-cancer treatment-induced complications, various strategies and standard-care treatment regimens are adopted by scientists and doctors especially for lung cancer patients. The clinical and biological aggressiveness of lung malignancies does not allow for anti-cancer therapy to be withheld or postponed, which may lead to the worsening of the disease.
Sine this pandemic situation has greatly affected the psychology of the patient, whether due to social stigma or the cause of abandonment, the patient needs a lot more care and support both physically and mentally. The patients must be managed in such a way that they do not get any unnecessary exposure to the virus that will help to flatten the curve of SARS-CoV-2. Hence proper management of the disease is the goal to reduce infectious heads.
Conclusion
Clinical research has slowed down as SARS-CoV-2 surged and took a turn to pandemic. It is necessary to investigate the susceptibility of lung cancer to SARS-CoV-2 at molecular levels and take basic precautionary and preventive methods. The risk factor increases in asymptomatic patients who spread the disease unknowingly to healthy individuals and develops the severity of the disease when diagnosed especially in comorbid patients. More strategies and patterns must be implemented to slow down the infectious rate of coronavirus.